(Daily Caller News Foundation) – Private emails from leaders of an influential transgender medical organization expose how ideology and consensus, rather than science, has undergirded the explosive growth of the child sex-change industry. The emails were revealed under Freedom of Information laws.
As their gender clinic boomed with patients, University of California San Francisco (UCSF) medical directors Maddie Deutsch and Stephen Rosenthal acknowledged behind the scenes that research supporting child sex-changes was “shoddy” and fueling “predatory practices,” emails show.
Deutsch and Rosenthal are leaders in the field of gender medicine and co-authors of the World Professional Association of Transgender Health’s (WPATH) highly influential medical guidance, the Standards of Care version 8 (SOC 8), which is used to inform clinical practice in healthcare systems worldwide. Rosenthal co-founded the UCSF Child and Adolescent Gender Center (CAGC) which had a “major backlog” of 230 new patients on waiting list in the fall of 2022, records show. Rosenthal said the staff’s capacity was “maxed out” and a colleague noted “the need far outpaces the access to care for gender diverse youth,” emails show.
When the Daily Caller News Foundation’s public record requests for Deutsch and Rosenthal’s emails were denied by the University of California in the fall of 2023, Judicial Watch, a government watchdog organization, filed a lawsuit challenging the denial and gained access to the records.
As a result of Judicial Watch’s lawsuit, UCSF released 2,491 pages of emails. Among the revelations is that UCSF gave puberty blockers to children as young as nine. Puberty blockers are not approved by the Food and Drug Administration for the treatment of gender dysphoria.
“There is something rotten in the state of California,” said Judicial Watch President Tom Fitton in a press release.

Shoddy Research
A May 2022 email obtained through the lawsuit accused Rosenthal and his gender clinic colleague, Dr. Diane Ehrensaft, of peddling “shoddy research” in a March 2022 op-ed published in the San Francisco Chronicle. The op-ed argued against legislative bans on child sex-changes and cited a highly criticized February 2022 study, authored by Diana Tordoff, as evidence that puberty blockers and cross-sex hormones significantly lowered depression and suicidality amongst gender-confused youth.
The flaws of the Tordoff study were brought to the attention of Rosenthal via email.
“You cite the Diana Tordoff study from Seattle Children’s Hospital as evidence of the ‘clear mental health benefits’ of gender-affirming care. Except that, apparently, that study says no such thing,” states the email. The name of the emails author was fully redacted.
“The same shoddy research is wheeled out again and again,” the message continued.
Rosenthal responded to the email by agreeing the study had “significant methodological concerns.”
“I completely agree with you about the Tordoff et al. paper, and wish that I had realized the significant methodological concerns,” wrote Rosenthal.
“We are still actively involved in our 4-site NIH study and now publishing articles on the impact of the first two years of gender-affirming care … I couldn’t agree more for the need for long-term follow-up, and that is exactly what we are committed to do,” Rosenthal wrote.
In September 2022, the Tordoff study was cited by WPATH in the SOC 8 as evidence supporting the benefits of child sex-changes.
Rosenthal was the co-investigator of a long-term National Institute of Health (NIH) study led by Dr. Johanna Olson-Kennedy on the mental health impacts of using puberty blockers as a treatment for gender dysphoria. Olson-Kennedy controversially withheld the results of the study, which showed puberty blockers did not improve mental health of gender-confused children, out of fear the data would be “weaponized,” according to reporting in October 2024 by The New York Times. A preprint of the study was published in May 2025.
WPATH, Deutsch and Rosenthal did not respond to the DCNF’s requests for comment.
Overlooking Risks
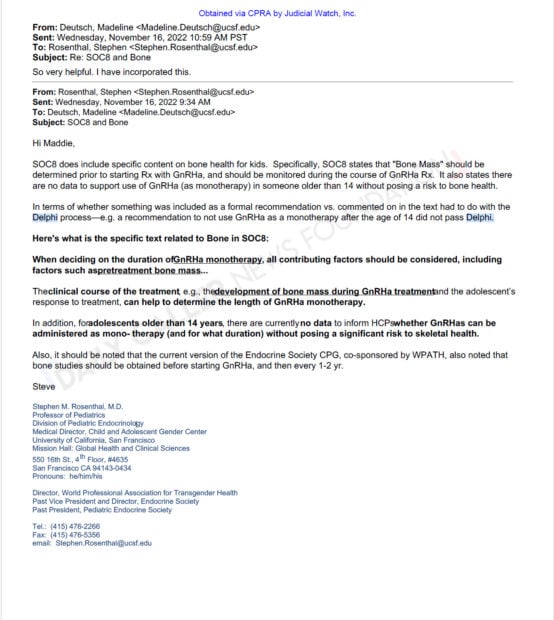
Rosenthal explained to Deutsch in a November 2022 email that giving adolescents over age 14 puberty blockers as a monotherapy, meaning without additional sex hormones, put the bone health of teen patients at serious risk, emails show.
“[SOC 8] also states there are not data to support use of GnRHa (as monotherapy) in someone older than 14 without posing a risk to bone health,” wrote Rosenthal.
Rosenthal stated WPATH did not include a recommendation against the risky therapy in the SOC 8 because it “did not pass” the Delphi process, a method to establish scientific consensus used by WPATH to determine what was included in its clinical guidance. Under the Delphi process, WPATH members anonymously voted for proposed clinical recommendation statements, rating them on a scale from 1 (strongly disagree) to 9 (strongly agree). Statements were included in the SOC 8 if at least 75% of voters rated the recommendation 7 or higher, according to WPATH’s website.
WPATH’s use of the Delphi method was “deeply flawed,” Dr. Kurt Miceli, medical director of Do No Harm, told the DCNF.
“WPATH’s use of the Delphi process to justify its guidelines on gender-affirming care is deeply flawed — not because of the method itself, but because of who was allowed to define ‘expertise,’” Miceli told the DCNF.
“When a consensus is built among ideologically aligned individuals who ignore conflicting evidence, the result isn’t science—it’s dogma dressed up as clinical guidance,” Miceli added.
A draft copy of an SOC 8 chapter on cross-sex hormone therapy for children and adults showed 12 0f the 21 proposed statements that passed the Delphi process were rated by WPATH as having a “low certainty of evidence,” according to documents from Boe v. Marshall released by Alabama Attorney General Steve Marshall.
Even Deutsch expressed doubts about the credibility of the Delphi process.
“I think that having the SOC8 be primarily focused on explanatory statements for the approved delphi statements is a misguided approach,” Deutsch wrote in a November 2021 email.
“Furthermore, most of the recommendation statements in SOC8 are not PICO format but consensus based or based on weak evidence. So it seems somewhat arbitrary to exclude other very important information and topics,” Deutsch continued.
The PICO process is a framework used in healthcare to formulate evidence-based research questions.
Fueling ‘Predatory Practices’
Deutsch also criticized the “lax approach to criteria for surgical care in general” WPATH was taking in the SOC 8, emails show.
“I wanted to emphasize the concerns I raised regarding the assessment chapter’s statement that the guideline for surgery access will be a ‘suggested’ 6 months of hormone therapy prior to permanent and sterilizing genital and gonadal procedures, as well as the general lax approach to criteria for surgical care in general. In my view and experience this is very inappropriate and will have several very negative effects,” wrote Deutsch.
“It will fuel already opportunistic and in some cases predatory practices by some surgeons in this field, who will be emboldened as well as enabled by a removal of any waiting period,” Deutsch continued.
Deutsch was concerned the lack of protocols when assessing gender-confused patients would be “opening up the tap” to “surgery on demand.”
“Will a surgeon themself be able to do the assessment if they so deem themself as qualified to do so? I am absolutely certain that, should this content remain as-is, within weeks of SOC8 release, there will be scores of new grad primary care nurse practitioners and PAs, who have completed 2 years of masters level training, identifying themselves as qualified to make these assessments and opening up the tap to what is effectively surgery on demand,” wrote Deutsch.

Shortly after the SOC 8 guidance was published in September 2022, Deutsch announced in an email that the UCSF gender clinic would be immediately implementing the lowered assessments standards.
“WPATH SOC8 is out and no longer requires a mental health ‘letter.’ So we can now focus on patient-centered assessments. A single ‘letter’ is provided by any qualified provider to attest to the patient’s need for and appropriateness for surgery. In general, this letter should be able to come from the treating surgeon,” wrote Deutsch.